Ebola, South Sudan Illness, and Coronavirus Update: 16 Dec 2021
Coronavirus ArchiveAs reminders…
Alpha–Variant first identified in the UK
Beta–Variant first identified in South Africa
Gamma–Variant first identified in Brazil
Delta–Variant first identified in India
Omicron–Variant first identified in South Africa

Also as a reminder:

Ebola–
There are no new cases of Ebola in the DRC, and all of the known contacts have cleared the incubation period. The WHO is on course to declare the official end to the outbreak in just a few days.
South Sudan Illness–
You have probably seen headlines about the WHO dispatching a team to investigate an outbreak of a mysterious, presumed communicable disease in a portion of South Sudan that has been hit by very heavy recent flooding. There are between 88 and 89 deaths attributed to this mystery illness, but I cannot find anything on the time frame of those deaths or even mention of symptoms at this point. I do know they have ruled out cholera (apparently I was not the only one with that first thought in this region, plus flooding), and that’s why the WHO team has been called out. Basically, very early days, details are very sketchy, and hopefully we get more clarity in the next week or two. Identification of the agent, or at least details on symptoms, would be helpful, if nothing else.
Coronavirus–
–In the UK, cases are rocketing up, including multiple outbreaks of endemically spread omicron. News and authorities in the UK have been slightly less reserved than their approach to the Blitz, but even there, hospitalization trends in available data appear promising. In the US, Indiana, at least, has leveled off the recent rise and is starting to come down on new cases. Still almost exclusively delta in Indiana, so hospitalization rates remain quite elevated. Indiana is one of four states in fact to have dialed up the National Guard to assist particularly hit hospital systems. Cases are also still elevated in much of the Great Lakes regions of the Midwest and the Northeast. The NBA and NFL are having trouble filling out rosters for occasional games as more players are popping positive on surveillance. I have yet to read about any of them being hospitalized yet in these recent outbreaks, so small blessings. But it’s not clear any one is asking that relevant question–I’m just presuming if it was happening, we would know because it would be instantly click-baity. Based on reports from sewer surveillance for COVID in wastewater (turns out to be a great leading epidemiology indicator for new case volumes in the following week), Boston is about to blow up, yo’. Cornell cancelled in person classes after an outbreak of positive tests in hundreds of students, despite a requirement for full vaccination for students and faculty. They are presuming omicron, and I don’t doubt it. I’m not aware of large numbers of hospitalizations from that outbreak though, but it did not appear that any reporters covering that story asked that very relevant question.
And they say journalism is dead.
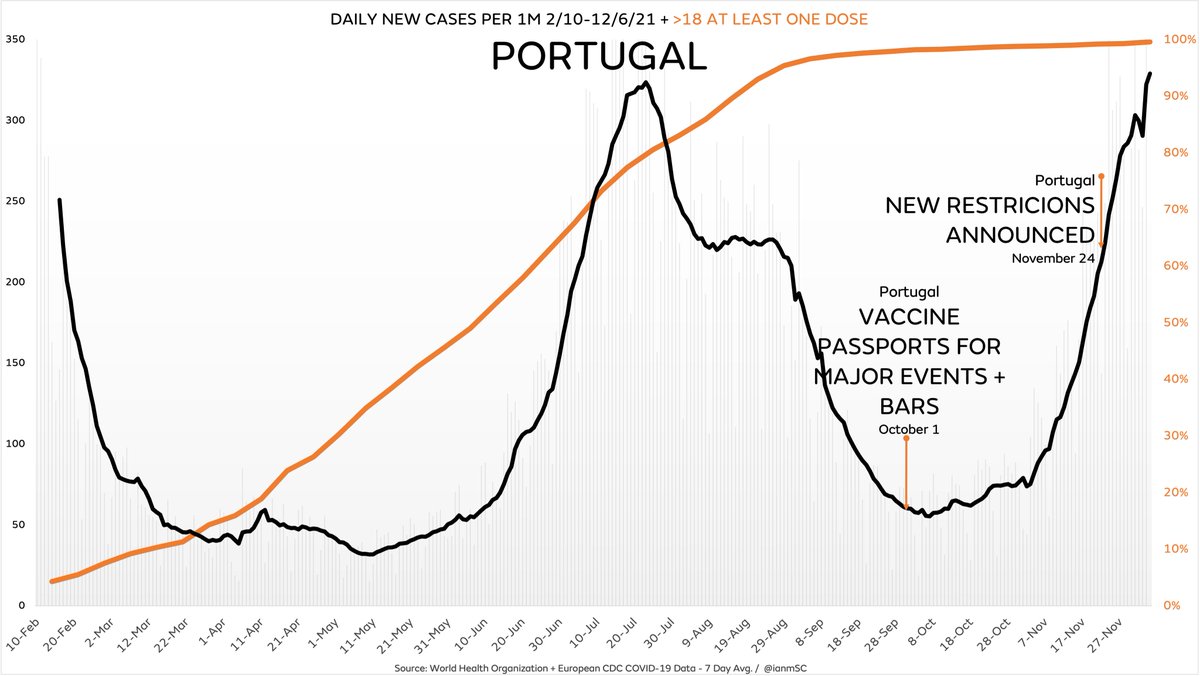
Anyways, we’ll get to South Africa in the more omicron specific portion. China is also seeing rising cases still, and is quarantining US and UK travelers no matter California has re-imposed a statewide mask mandate, New York is demanding proof of vaccination for 5 year olds to enter restaurants, Australia is using its COVID internment camp/treatment centers, and because we somehow live in the introductory paragraph of a Charles Dickens novel, you have at the same time headlines about how high vaccination rates, masks even vaccine passports have not slowed the spread in areas like South Korea, Portugal etc.
Which of those best of times, worst of times stories you saw depends largely on the preferred narrative of your preferred news source, as usual. Remember, why am I reading this? Why now? How does this make me feel? Why do they want me to feel this way? And yes, we do note, even before getting to the socioeconomic section that YouTube and Facebook have announced more aggressive enforcement of vaccine misinformation, including the absolutely true, albeit reduced probability of, spread of COVID by those who have been vaccinated, especially if symptomatic with a breakthrough case. This in the same week that Facebook argued in court that its “Fact Checks” were not statements of fact fact, per se, but instead constitutionally protected opinion.

–In omicron news, the UK confirmed –a– death from omicron (among well over 1,000 known cases), but has given no other clinical details about this case as of the time I am typing this.
–The big omicron news this week though was updates from South Africa looking at real world performance of the Pfizer vaccine there. As a reminder, Pfizer’s mRNA vaccine is the most commonly used vaccine in South Africa, particularly in areas hit hard by known omicron cases. By their reported estimates, the Pfizer vaccine is only 23% at preventing transmission of SARS-CoV-2 omicron. However, symptoms appear reduced in the vaccinated and most importantly, hospitalization is reduced by 77% with a full vaccine series. While that is the lower end of hospitalization prevention estimates for the Pfizer vaccine versus the other variants, it is worth mentioning again that hospitalizations in general from omicron have been less intense and have not lasted as long versus other variants in these regions of South Africa as well.
–Indeed, there is every indication that Guateng, the part of South Africa with the cluster that started the identification of omicron, has already peaked new cases. Most of these are suspected or confirmed omicron. While hospitalizations and deaths are lagging indicators, the per capita rate of both versus previous variants (delta especially) is much lower with omicron.
–More contagious, less severe, and good protection from hospitalization/death with vaccination is the scenario that is still very much in the lead, and building steam. That said, I think there is growing reason to suspect a higher rate of breakthrough mild infections with omicron in those already vaccinated. But again, that does not appear correlated to an increase in hospitalization.
–Speaking of breakthrough chances, we have another large, well conducted study in Israel on a different database from previous papers from Israel that showed natural immunity may be more protective than vaccine induced immunity. You can find the pre-print here. The money data is here:

So what you are looking at there is infection rate per 100,000 at risk days based on whether you got naturally infected and recovered (A. graphs above), got a vaccine +/- a booster (B., booster is green) or hybrid immunity which is natural infection followed by vaccine OR vaccine followed by breakthrough (C., with vaccine then breakthrough in purple at bottom). The Y-axis is time from that event, so “Vaccinated 2-4 months” is the risk of a breakthrough per 100,000 risk days for those whose vaccine was complete 2-4 months ago.
ALSO NOTE THAT THE SCALE IS DIFFERENT IN THE Y-AXIS GRAPH FOR A. The bottom graph in A. is for those who were infected and recovered from COVID 12+ before, while vaccine and hybrid scales max out at 8 months.
So what does this show? At 6-8 months post recovered natural infection or post vaccine, breakthrough infections were ~9 times LOWER in patients with natural infection. This is consistent with previous reports from Israel. As we covered before, this is at odds from the CDC’s conclusion. Could be differences in patients, but this replication of findings on an independent data set raises the chance that CDC’s data is the outlier here.
Interestingly (remember to pay attention to time scales!), at 6-8 months, hybrid immunity (combination of vaccine AND a recovered infection) is approximately equal to just recovered natural infection. The trend for slightly higher risk if you got a vaccine first THEN recovered from a breakthrough infection may be real, but does not appear statistical significant in this data set, and would need a whole lot more cases to show that its not just random chance.
In short, what they show is that there does appear to be a higher risk of breakthrough the further out from vaccine you are, although I really wish antibody testing were more routine to establish who really needs a booster (beyond those who have significant risk factors who should be getting a booster regardless). The booster may reduce that risk, but again, you may be confounded here as those lining up for early boosters were probably also doing other things to reduce their risk as well versus the other categories of patients.
–Speaking of boosters, thank you to the fellow physicians on the reader list, some of whom have reached out after the last couple updates. Between them and talking to other physicians in person around here, I am anecdotally struck by a few things. Many of my fellow docs are also finding ways to get their antibody levels drawn. All of the ones with high antibody levels have been deferring the booster based on their antibody titers. Small N, but it’s seriously 100% of those with titers through the roof, most of them also a year out from vaccination. So I don’t think I am the only doc waving the “we need to be using antibody tests more frequently to help guide patients without major risk factors in their decision to get boosters!” flag. Especially since there have also been some anecdotal reports back to me of still rare, but still happening, autoimmune like reactions after boosters.
–Also on a medical note, one of those reader docs prescribes a lot of CPAPs and confirms the major CPAP shortage due to difficulty sourcing chips for them.
If you, or someone you know, has a CPAP they no longer use, YES, they can be refurbished for those who need them, and YES, they are needed.
You can find more on how to do that here (they might also be a tax deduction) at this link or this link. Please spread the news around.
–No, I did not listen to the JRE where Joe Rogan had Dr. Peter McCullough on. I did skim the transcript though. Dr. McCullough is a well published cardiologist. As an academic clinician, he has more degrees of freedom to be more direct on his opinions than I can be. His points on using PCR to test asymptomatic patients being less than ideal, the need to exclude flu and other similar clinical overlap viruses when diagnosing COVID, death certificate conventions (did they die of or with COVID), and especially preventing hospitalization as the key metric are all topics that should be very familiar to readers of these updates. He also describes the pathology as viral infection followed by immune freakout which leads to clotting in some patients–this is also familiar turf to readers. He is a little more direct in his questioning the emphasis on vaccination and the apparent lack of emphasis on treatment. He discusses early treatment options. I have to tread carefully there, and thank you for your understanding. I will say I think he is a little quick to ascribe to malice that which is best explained by stupidity (as he quotes one of his friends closely working with major institutional players, describing what the friend believed was their “incompetence.”) He gets close to New World Order-y about the vaccination drive, when again, I think the best explanation is simply politics. A politician seeks to be perceived as effective. Vaccines out are easy to count, and “everyone knows” vaccines worked because it’s how humanity curb stomped polio and small pox. So I think the political emphasis is the universal desire for politicians to appear effective, to have to decide absent deep expertise in the medical matter or with incomplete information, coupled with the very human foible that we hate to admit when we are wrong.
As anyone who has ever argued with a spouse or significant other can attest.
Of course, we are all wrong a LOT. There is no shame in it. But the feeling of that shame, and wanting to avoid the bad feeling, is universal. So a politician who comes out hard in the paint on something like a vaccine passport, for example, is going to be slow to walk that back. Both for the individual “avoid the bad feels” factor and the concern that opponents will pounce on them for waffling or “being weak.” Of course they are right, but they are damned if they do and damned if they don’t because honestly, the politicians of every tribe and type will absolutely find fault no matter what decision someone they oppose makes. That’s why there are entire Twitter archives of very serious political people who would “never take a rushed, unsafe Trump vaccine!” who will now tell you on the same Twitter that you are murderer for not getting a booster yesterday. And there is equal cognitive dissonance on the other side–don’t read too much into one example. But that’s why. It doesn’t matter what decision you make–the other tribe’s narrative machine is LOOKING for schismogenesis and will always find it, even if they have to twist themselves in knots too. You’re better off admitting the situation has changed, the science has changed, the data has changed, and so your decision and policy has changed. But that kind of wisdom is not as common as it really should be. Humanity has a bad habit in general of selecting its leaders for their ability to score points on the other team, not necessarily for the real wisdom of the leaders.
The world around us is the predictable result of that criterion, unfortunately.
Anyways. In short, I think from what I skimmed he is making some observations we have covered here a lot. He’s just a little closer to the conspiranoia line than I am. So some good stuff, stated stridently and for max emotional impact, and some that is probably overstating ill intent and conspiracy.
Socioeconomic–
–The Bureau of Labor Statistics announced that it will change the baseline for the Consumer Price Index, which measures inflation, beginning in January 2022. Brief, cryptic, and largely unnoticed announcement here.
–A Nobel prize winning economist famous for damn the inflation, full print ahead policies mused on Twitter this week if inflation really hurts the little guy, even when prices rise faster than their wages and they can afford less of the little they could afford already. Our economist was nuked from orbit in the replies like civilians in Syria around US drones; sorry is this too soon, or doesn’t count because no one has even been reprimanded for these disasters let alone the one in Afghanistan recently?. Because yes. Yes it does hurt the little guy.
–Shockingly, congressional leaders did not find an issue with congressional leaders trading stocks on insider information or which will be regulated by the laws they are about to vote on.

–Why the labor shortage everywhere? Re-thinking of priorities is part of it. LinkedIn reports the number of remote positions has doubled, and people are 25% more likely versus 2019 to be looking for a new job. Early retirements and exiting the labor market for caregiving responsibilities, from more time at home with the kids to elder care, play a big role too. There are estimates of 1 million workers dropping from the work force for such re-prioritization choices already. On top of that are estimates of up to 197,000 extra working age people who have either died or have had some form of disability from severe COVID.
And that is not counting knock on effects from the reaction to the pandemic. We know that drug overdoses and abuse/addiction issues increased during the pandemic. Just for some quick stats on that:

This had effects on homelessness, with meth in particular showing a strong linkage. On top of that, you had increases in mental health issues and diagnoses. You have seen these headlines throughout the pandemic, and this is just the most recent, focusing on adolescents and young adults. The same applies for older demographics too though. Lastly, we mentioned a few weeks ago that ERs were also being stressed by non-COVID admissions, usually for chronic diseases that were going undertreated as people avoided going to the doctor’s office as often (or the doctor’s office was closed during periods of high COVID transmission, converted to acute COVID care instead).
The long story short of all of that is the number of effective working age people has dropped, probably more than we realize at first blush until we add up all those potential causes.
Employers may also be partially to blame, as this article hypothesizes, including some post-COVID world reasons.
Anyways, some possible explanations to keep in the back of your mind as you wonder where everyone is with the seeming never ending staff shortages all over…
–Several major national healthcare chains have dropped or moved vaccine mandates for fear that enforcement would exacerbate labor shortages. Elsewhere, the CEOs of Southwest and American Airlines made headlines this morning questioning the need for masks on planes, arguing that the HEPA filters on most planes adequately remove most pathogens, during testimony to Congress on the airline industry after all the billions the country pumped into it during shutdowns last year. The PR team for at least one of those airlines was out almost immediately in spin control to minimize those statements. Kroger this week announced that not only was it ending COVID pay, but unvaccinated employees would be hit with a surcharge for their health insurance. That’s a bold move, Cotton, because one wonders if they are doing the same for smokers, or people they don’t think exercise enough etc. who also likely incur increased health care risk. Demographically, again, that surcharge is a little more likely to land on employees of ethnic groups with damn good historical reason to NOT trust a government run vaccination campaign as well, and that won’t be a real great look for Kroger. Elsewhere, I am sure you are seeing the same headlines I am about varying degrees degrees of draconian enforcement of vaccine mandates etc. around the world. Your local level of restriction will definitely vary.
–Finally, your think pieces on the US healthcare system. Or “a big part of the reason your author left clinical medicine”. Both are worth reading in their entirety: Scripps “mastercharge” mark ups leak. We had a lecture from a payment guy in the hospital system I was at during residency, because pathology actually does need to know about the billing (hospitals tend to view us as a giant cost center, so you are constantly having to justify to administration why the lab is needed, and how the tests save on costs overall across the system). I know how they decide what mastercharge to apply, and the rationale for it is stunning across the board. Ask me about it some other time though. The other one is here. There is a section where they throw out example dollar numbers. Follow the money, and see what everyone is making in the scenario with, and without, the middlemen. And the study by the University of California that is mentioned will surprise you.
–Your chances of catching Ebola are equivalent to the chances that if a system is opaque and too complex for any one party to understand, it will work fairly and equitably for the average consumer of that system.
–Your chances of catching South Sudan Illness are…

–Your chances of catching coronavirus are equivalent to the chances that a system which is too complex for any one party to understand, and has a lot of parts that don’t seem to make any sense, is that way for a reason–because it benefits someone. And the chances are that someone isn’t you.
<Paladin>